In this presentation, Dr Strober provides us with new data on TNF alpha inhibition in the treatment of hidradenitis suppurativa (HS). HS is sometimes referred to as acne inversa; however, Dr Strober feels it is a different disease based upon a lot of lines of evidence.
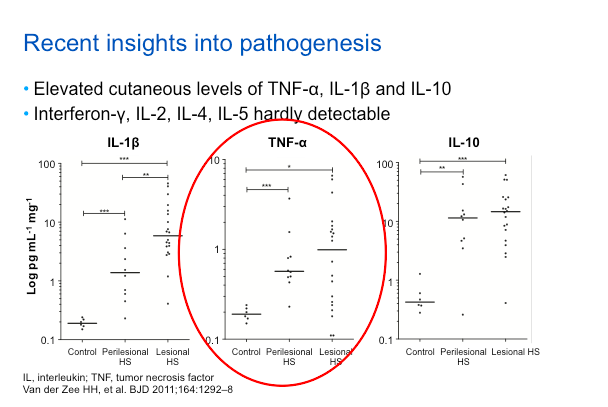
Based on recent insights into the pathogenesis of this disease, TNF inhibition has found to be an effective treatment. Essentially, it’s phenomenological, because if you look at lesional skin, there is more TNF alpha as compared to peri-lesional as compared to control skin. This isn’t to say that TNF is the only relevant cytokine; in fact, it may be the first of many which will be targeted over the next decade. Just like in psoriasis, TNF will be the first cytokine studied for targeting in HS.
Etanercept
Overall, etanercept (ETN), at the doses that have been studied, does not appear to be effective treatment for HS. The prospective, double-blind, placebo-controlled trial of 20 subjects were randomized 1:1 for ETN 50mg BIW versus placebo for 24 weeks. The primary efficacy endpoint assessed the Physician Global Assessment (clear or mild). Secondary endpoints included change in Patient Global Assessment and quality of life (DLQI). The results demonstrated that there was no statistically significant difference in benefit between ETN and placebo. There are some case reports that also verify this phenomenon.
Infliximab
The case reports for infliximab, which were published several years ago, showed efficacy in the treatment of HS; however, many patients had concomitant IBD, which is not uncommon among patients with HS.
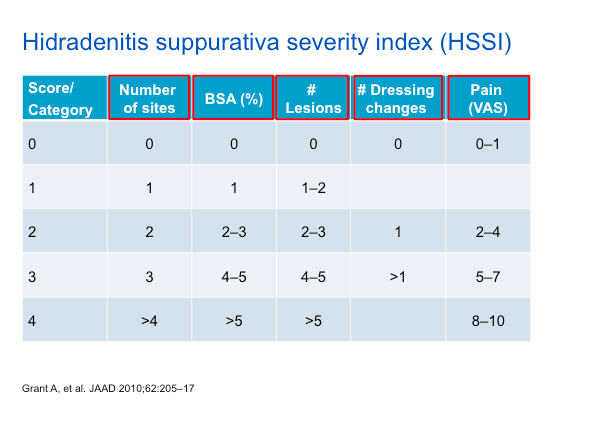
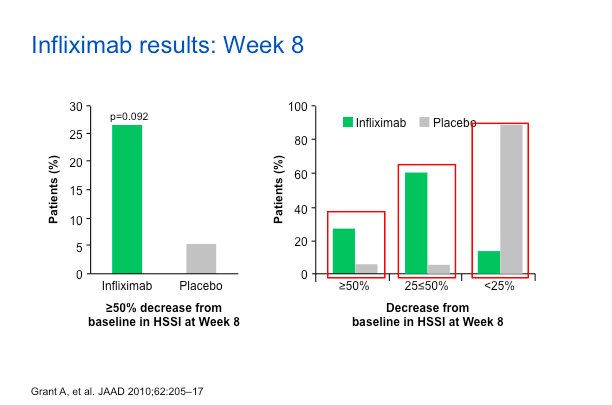
A prospective, double-blind, placebo-controlled trial of infliximab IFX) included 38 subjects randomized to either IFX or placebo. The study’s primary endpoint was a 50 percent reduction in HS Severity Index (HSSI) at week 8 and secondary endpoints included change in Visual Analog Scale (VAS) and DLQI.
As noted in the table above, the HSSI score takes into account a variety of features, including dressing changes and pain—which are aspects of the HS experience that should be queried with each patient.
As we can see, about 25%-30% of patients on IFX have a reduction in HSSI score versus the placebo group. If you look at the 25%-50% reduction range, you can still see a bias towards IFX. Dr Strober feels that these are good data substantiating the value of IFX for the treatment of HS.
The VAS score as well as DLQI also show that IFX did better than placebo.
Dr Strober has used IFX on at least forty patients and feels that it really is the best drug out there, if you can access it. He also recommends using it with methotrexate to sustain the effect of IFX.
Adalimumab
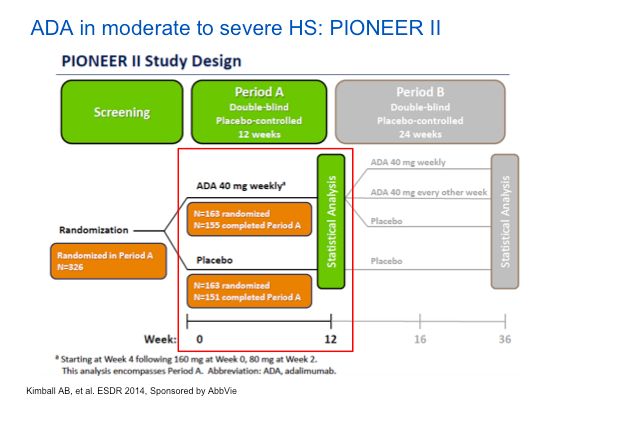
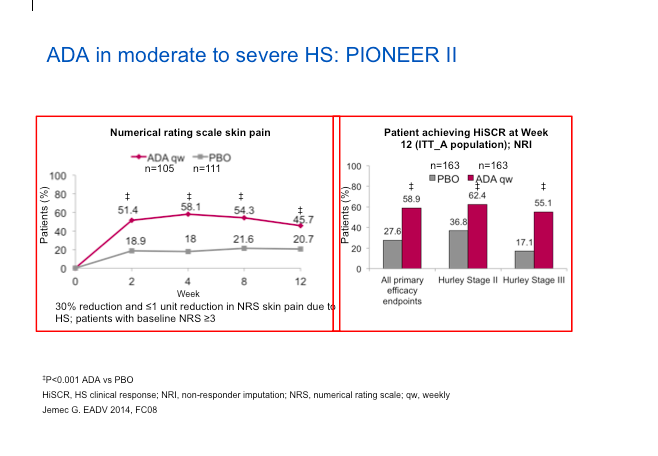
Adalimumab (ADA) represents the best set of studies done to date for the treatment of HS. The PIONEER II study looked at the safety and efficacy of ADA versus placebo in patients with moderate-to-severe HS after treatment for the first 12 weeks. The endpoint involved counting abscesses and inflammatory nodules. The HiSCR score, which Dr Strober feels is a valid score, is not dissimilar from other endpoints, in that it measures relevant issues in HS.
The study design was rigorous, in that they did a randomized, placebo-controlled approach. They key point here is that ADA will be dosed weekly, not every other week as it is when treating psoriasis. The phase II studies showed that ADA every other week did not perform as well.
Interestingly, many more women were enrolled in this study than men. Also of note, is that two thirds of the patients in the study were smokers. Remember that HS is a systemic, inflammatory disease. Much like psoriasis, we should think of it as a systemic syndrome of inflammation.
When we look at the data (below), we can see the numerical improvement in the rating scale of skin pain is biased towards ADA versus placebo and we can see more people achieving a HiSCR on ADA versus patients on placebo.
The ADA group also does better with regard to inflammatory lesion count reduction as well as the Sartorius Score reduction.
The safety data are remarkably clean in these studies, particularly focusing on infection, serious infection and malignancy. If anything, there were more events in the placebo group.
Clinical Pearls
What do we need to remember about HS?
HS is a chronic, negatively life-impacting disease.
Associated with metabolic syndrome (obesity, DM, HTN, dyslipidemia)
Pathogenesis multifactorial; primarily inflammatory and not infectious, and our understanding is evolving
Phase II/III studies with adalimumab are the best studies, to date, and convincing of efficacy and good safety
Infliximab also is very effective
MauiDerm News Editor-Judy L. Seraphine, MSc
https://mauiderm.com/wp-content/uploads/2013/04/MD-WebLogo.jpg00Maui Derm Newshttps://mauiderm.com/wp-content/uploads/2013/04/MD-WebLogo.jpgMaui Derm News2015-06-01 03:20:502015-06-01 03:20:50TNF-a Inhibition and the Treatment of Hidradenitis Suppurativa
Genetic advances are teaching us more about psoriasis as a disease state. The discovery of pathways that influence psoriasis have led to treatments such as TNF alpha inhibitors, interleukin-23 inhibitors, and IL-17 and its receptors. We have also learned that CARD14 mutations are a cause of familial psoriasis/PRP. One of the ways that CARD14 works is through the activation of IL-23 signaling and Th-17 expression, leading to the use of ustekinumab, a commercially available agent that targets IL-12/-23 with success.
Through exome sequencing, we have learned more about generalized pustular psoriasis. There is a deficiency of the interleukin-36 receptor antagonist, DITRA, in hereditary pustular psoriasis (and some cases of “sporadic” generalized pustular psoriasis show mutations in the IL-36R antagonist). This discovery suggests that activated IL-36 (or its related compound, IL-1) may be an important target in pustular psoriasis.
What about alopecia areata? We have learned from some excellent genome-wide association studies (GWAS) that there are several loci that are increased in this disease, one is which is CTLA4. There are ongoing trials of abatacept (CTLA4-Ig initiated) and rixolitinib (JAK 1/2 inhibitor to suppress IL-15 activity), but an early report of JAK1/2 inhibition showed great promise.
Targeting Functional Pathways
We can use systemic administration of small molecule inhibitors to suppress signaling activation. This can be seen with the use of vismodegib in basal cell carcinoma and basal cell carcinoma syndrome (BCNS) (activation of hedgehog signaling) and oral rapamycin in tuberous sclerosis (activation of mTOR signaling). GNAQ mutations cause the majority of blue nevi and 90 percent of cases of Sturge-Weber syndrome and nonsyndromatic portwine stains. GNAQ mutations have now been shown to activate PKC and MAPK but not AKT or mTOR. This observation suggests that an inhibitor of PKC or MAPK signaling might be effective if applied topically. With epidermal nevi, activating mutations have been detected in the genes encoding RAS family members or affecting FGFR3/PI3K/AKT signaling. Differentiating the activated pathway could influence decision-making about the most appropriate inhibitor to apply topically in the future. G13R and Q61R or Q61L Hras mutations in melanocytes cause Spitz nevi and speckled lentiginous nevi, yet another situation in which a targeted inhibitor which blocks Ras signaling might be considered as therapy.
Protein Replacement Therapy
Intradermal or intravenous introduction of recombinant collagen VII into RDEB (recessive dystrophic epidermolysis bullosa) mice leads to the deposition of collagen VII at wound BMZ and decreased skin fragility. Recently, FDA approved a trial of injected collagen VII in patients with RDEB. Future investigations might involve topically applied recombinant collagen VII to wounds or even intravenous delivery to reach mucosal sites as well. Interestingly, studies in mice without epidermolysis bullosa suggest that even normal wounds heal more readily if collagen VII is administered, broadening the potential value of topically delivered collagen VII.
Replacement; however, may not be sufficient. In CHILD syndrome, the cholesterol biosynthetic pathway is blocked, leading to deficiency of cholesterol but also accumulation of toxic metabolites. Application of topical cholesterol to skin is not sufficient, but use of a statin to block both the accumulation of toxic metabolites, as well as replacement of cholesterol leads to dramatic improvement in affected skin using this “pathogenesis-based” therapy.
Summary
New technology has facilitated the advancement in our knowledge about gene function and the effects of gene alteration, including for some of the mosaic disorders. These discoveries have translated into new therapies for patients with genetic disorders and will help with innovative treatment in the future, whether personalized gene-based or pharmacologic therapy. While there are new discoveries to be made, one of the exciting new frontiers involves epigenetics—unraveling how and why genes are turned off with cell and tissue specificity – and then translation this information towards treating human disease.
https://mauiderm.com/wp-content/uploads/2013/10/Paller-PHoto.jpg12521100Maui Derm Newshttps://mauiderm.com/wp-content/uploads/2013/04/MD-WebLogo.jpgMaui Derm News2014-12-12 00:36:512014-12-12 00:36:51Applying Laboratory Breakthroughs to Treat Pediatric Skin Diseases: Part 2
Dr Gupta, an expert in the management of nail disorders, discusses clinical advances with regards to the management of onychomycosis.
Factors Affecting Diagnosis
It is very important that we correctly diagnose onychomycosis. For the first time in over twenty years, we are able to use techniques other than light microscopy and culture. Molecular biology can be used to accurately diagnose multiple organisms that may cause onychomycosis. Dr Gupta has learned, through his lab, that often we may have mixed infections of two dermatophytes, a dermatophyte and a non-dermatophyte, or two non-dermatophytes. PCR analysis is more sensitive than culture, so it has a greater ability to identify mixed infections.
Treatment
Oral Therapies
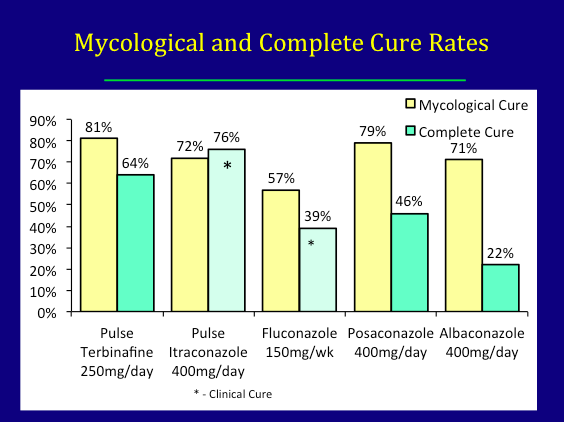
Onychomycosis can be managed with topical therapy, oral therapy, and/or devices, i.e., lasers. In terms of oral therapy, terbinafine is the gold standard. Itraconazole is also indicated for the treatment of onychomycosis and fluconazole can be used off-label.
There are two new oral drugs in development—posaconazole and albaconazole.
It is important to recognize that onychomycosis is a difficult disease to treat, so you should consider the fact that you may need booster therapy or extra treatment around six to nine months from the start of therapy. For example, with terbinafine, giving 250mg per day for four weeks and repeating that at nine months and twelve months.
Topical Therapies
Efinaconazole, a triazole, which was just approved in Canada, has a low MIC for dermatophytes, yeasts and non-dermatophyte molds and relatively low keratin binding to facilitate transungual penetration. With regards to mycological cure and complete cure, data for efinaconazole demonstrated 54 percent and 17 percent cure rates, respectively versus 32 percent and seven percent, respectively with ciclopirox.
Tavaborole, a broad-spectrum benzoxaborole antifungal, has a low molecular weight and low lipophilicity facilitating penetration into the nail plate. At week 52, tavaborole demonstrated a 34 percent mycological cure and an eight percent complete cure as compared to 32 percent and seven percent, respectively with ciclopirox.
We need to recognize that there are differences in the severity and population of participants between the studies looking at the efficacy of efinaconazole and tavaborole; therefore, precluding a head-to-head comparison.
Differences Between Efinaconazole and Tavaborole in Pivotal Phase III Studies
No upper age limit for tavaborole
Nail trim: tavaborole allowed no more than 1mm nail beyond hyponychium
Japan not included in tavaborole study
Efficacy of vehicle for efinaconazole 2x that of tavaborole
Luliconazole is a topical imidazole approved in the United States for the treatment of tinea pedis. There are phase II/III trials currently underway studying its efficacy for onychomycosis.
Device Therapy—Lasers
There is insufficient data to determine if lasers are fungicidal in onychomycosis, especially as the precise mechanism of action remains unclear. The most likely effect is a selective photothermal effect, although we cannot rule out a photoacoustic, photochemical, or photomechanical effect. Keep in mind that the fungus has to be heated to at least fifty degrees centigrade for at least ten to fifteen minutes or 60 degrees (or even 70 degrees) for shorter periods of time. The aim of selective photothermolysis is the create very high increases in temperature in the fungi while the water content in the dermis and the blood vessels surrounding the nail bed allows for the dissipation of heat to prevent pain and tissue necrosis. The pulse format of the laser is critical for ensuring that heat remains confined and elevated in the fungi, while providing sufficient time for the surrounding tissue to dissipate the heat,
In the United States, the division of the FDA that approves lasers is different from the division that approves anti-fungal treatments. Lasers are indicated for use for the temporary increase of clear nail in patients with onychomycosis—this is quite a different approval as it is a cosmetic approval that does not look for mycological or complete cure. These lasers have not been subject to the same stringent standards that we expect of topical and oral therapies. There have been a number of open, single assignment clinical trials conducted using laser systems; however, randomized, controlled studies are needed to determine if laser is an effective treatment
Prevention of Recurrence and Reinfection
Recurrence rates can be anywhere from 11 to 35 percent or even higher. Remember that fungi can be transmitted to uncontaminated clothing in the wash. It is important to remind patients to wash their clothes and shoes in hot water (greater than 60 degrees) for more than 45 minutes. Ozone can be used to sanitize shoes and sports equipment of dermatophytes, yeasts, and non-dermatophyte molds. Ultraviolet light can also be used to sanitize shoes and reduce fungal burden.
Factors Contributing to Recurrence and Reinfection
The fungus that causes onychomycosis is not just dermatophytes or non-dermatophytes, but mixed infections as well. We have also shown that T. rubrum is not just T. rubum; there are minute-based pair differences that produce different strain types. We have found that strain type switching may contribute to the failure of oral terbinafine.
In summary, terbinafine remains the gold standard for treating onychomycosis. Both continuous and pulsed regimens are beneficial with an optimal pulse regimen of four weeks on, four weeks off and four weeks on. We have found that using this strategy, taking into account the pharmacokinetics of the drug, we can achieve fairly high cure rates. Itraconazole 200mg melt extrusion tablet may lead to better compliance rates versus two 100mg capsules. Don’t forget about booster therapy!
Fluconazole, while off-label in the United States, can be used at 150mg/week for longer than six weeks is also effective. The efficacy for posanoazole and albaconazole is similar, but not superior, to that of terbinafine.
We also have new topicals for onychomycosis—efinaconazole and tavaborole. It remains to see whether or not they will be used as monotherapy or in combination. Perhaps they could be effectively used in patients who fail oral terbinafine. They may also be used to prevent early recurrence of onychomycosis. There are a lot of potentials for the topical therapy.
As dermatologists, we use lasers for many things. We still don’t know enough about the use of lasers for the therapeutic cure of onychomycosis.
https://mauiderm.com/wp-content/uploads/2013/04/MD-WebLogo.jpg00Maui Derm Newshttps://mauiderm.com/wp-content/uploads/2013/04/MD-WebLogo.jpgMaui Derm News2014-12-12 00:32:062014-12-12 00:32:06Infectious Diseases: Update on the Management of Onychomycosis
Dr Blauvelt provides us with the 10 most important take-home messages from his immunology presentation at MauiDerm NP+PA Summer 2014….
Key features of the innate immune system include: rapid response, non-specificity, phagocytosis, no memory.
Key features of the acquired immune system include: slow response, very specific, lymphocyte-mediated, memory.
Keratinocytes are active participants in generating immune responses by secreting numerous cytokines upon activation.
4.Toll-like receptors are pattern recognition receptors on keratinocytes that recognize foreign antigenic material.
Antimicrobial peptides are natural antibiotic molecules found in skin that are abundant in psoriasis skin and sparse in atopic dermatitis skin.
6.Epidermal Langerhans cells are antigen presenting cells that recognize/process skin antigens and migrate to lymph nodes, where they present antigen to T cells.
7.T cells require 3 signals to become fully activated: 1) recognition of antigen by the T cell receptor via MHC on the surface of antigen presenting cells; 2) binding of co-stimulatory molecules on T cells and antigen presenting cells to one another; and 3) secretion of soluble cytokines by the T cells.
CD4+ T cells are T helper cells that recognize antigen via MHC class II and secrete cytokines to enhance CD8+ T cell and B cell immune responses, whereas CD8+ T cells are cytotoxic T cells that recognize antigen via MHC class I and kill cells upon contact.
B cells secrete antibodies that specifically bind to antigen.
Primary immune responses are slow, occur after first exposure to antigen, and involve creation of memory cells, whereas secondary immune responsesare fast, occur after subsequent exposures to antigens, and involve reactivation of memory cells.
https://mauiderm.com/wp-content/uploads/2013/10/Blauvelt-Pic.jpg480480Maui Derm Newshttps://mauiderm.com/wp-content/uploads/2013/04/MD-WebLogo.jpgMaui Derm News2014-07-02 02:24:032014-07-02 09:56:23Immunology 101: The Basics
At MauiDerm NP+PA Winter, Dr Zone provided the audience with some key takeaway points regarding systemic therapy….
What Does Dr Zone do with his Patients on Systemic Steroids??
Patients on systemic corticosteroids should be tested (prior) and monitored for hyperglycemia and hypertension—many patients’ blood pressure will skyrocket on systemic corticosteroids. Gastric ulcer protection may be provided with H2 blocker or PPIs as many patients will get ulcerative changes in their stomachs. These patients should be monitored every two to three weeks.
Dr Zone also utilizes osteoporosis prophylaxis for patients on systemic corticosteroids. That should include bisphosphonates, calcium calcium carbonate plus D, calcitriol, estrogen, or testosterone. The reason for this—if you start a patient on prednisone today, there is an excellent chance that the bones will start to demineralize immediately. When prescribing corticosteroids, start high to get control of the disease or symptoms, and then begin to minimize the dose. Give entire dose in the morning or bid early in the day. Alternate day therapy prevents adrenal suppression but NOT osteoporosis.
Taper oral corticosteroids in order to avoid rebound in cases of short-term treatment….In long-term management, slow tapers are important for dealing with adrenal suppression—the last 5mg is the crucial time for coming down slowly.
What about? Intramuscular triamcinolone—Dr Zone has been using this more in his practice. He finds that the patients have fewer side effects; sometimes they have trouble sleeping.
MauiDerm News Editor-Judy Seraphine
https://mauiderm.com/wp-content/uploads/2013/04/MD-WebLogo.jpg00Maui Derm Newshttps://mauiderm.com/wp-content/uploads/2013/04/MD-WebLogo.jpgMaui Derm News2014-04-30 01:00:342014-04-30 01:00:34Clinical Pearls: What to do with patients on systemic steroids?
Dr Zone has treated over one thousand patients with Dermatitis Herpetiformis (DH). It usually presents as itchy, red bumps in the elbows and knees. DH should be diagnosed through a biopsy and Dr Zone recommends biopsying in the area close to redness, but not directly on the red bumps.
There have been several studies looking at the prevalence of DH. The numbers in Europe are very similar to those of the United States. It is a genetic disease but it is distributed throughout life. We don’t know what the factors are that set off the onset of disease. We do, however, know that people with DH express the entire range of intestinal abnormalities. Some people will have Grade IV and others will only have Grade I.
Dr Zone stresses another important point that people with DH develop antibodies to epidermal transglutaminase (TG3). Dr Zone states that roughly one in six celiac patients will develop DH.
What about people who have intestinal inflammation, but don’t have DH or symptomatic CD?
It is important to consider that celiacs may have:
Only aphthous stomatitis
Only eczema
Only alopecia areata
Only psoriasis
Diabetes
Only fatigue or anemia
What this means is that all of the diseases mentioned above might be associated with celiac disease, it is pretty rare, but those people who have it might get better on a gluten free diet.
A 1998 paper studied oral ulcers and celiac disease. They found that approximately five percent of patients with “idiopathic” apthous stomatitis have been found to have positive endomysial antibody tests and then CD on small bowel biopsy. Stomatitis will clear with a gluten free diet. (Jokinen J et al: Celiac sprue in patients with chronic oral mucosal symptoms. J Clin Gastroenterol.1998; 26:23-26) In a 2008 study, the researchers looked at 269 kids ages 3 to 17 with CD and 575 otherwise healthy subjects. They found apthae in 61 of the 269 kids (22.7%) and 41 of the 575 normals (6%). 33 out of 46 CD kids on a strict gluten-free diet reported significant improvement or clearing of apthae. (Campisi et al. Dig Liver Disease. 2008 40:104-107)
Alopecia Areata (AA)
Alopecia areata is a T-cell mediated disorder that produces hair loss. Some studies have shown that patients with AA and CD have regrown hair with a gluten free diet (GFD) others have seen no effect of GFD. Also of note, chronic diseases can make the response to a GFD less likely. Dr Zone states that there is probably about one in 100 chance of having celiac disease. The questionable association between CD and AA and hair regrowth will only be answered by a prospective trial of testing new onset AA kids for total serum igA and tTG, establishing CD rate, and then comparing the outcome on GFP compared to non CD kids on a normal diet.
CD and Psoriasis
Take Home Point—CD occurs at a slightly increased frequency in psoriasis patients and response to a GFD has been reported.
A 2002 study of patients with long standing psoriasis who were found to have CD all had marked improvement on a GFD. Psoriasis patients with positive anti-gliadin antibodies have improved on a GFD. The prevalence of positive EMA and tTG antibodies is no greater than the rest of the population (1:133). The question is “is gluten a source of chronic antigen stimulation in psoriasis?” (Cardinali et al. Br J Derm. 2002.147:187-188)
CD and Atopic Dermatitis
There is no increased incidence of atopy in CD patients but patients with dermatitis who are shown to have CD will improve on a GFD. This was a large case controlled study of 82 CD patients and 180 matched controls and their first-degree relatives. The researchers found increased prevalence of asthma, eczema, rhinitis, or elevated IgE levels. However, patients with eczema and Cd did improve their eczema on a GFD. (Greco L, et al. Paediatr Scand. 1990 79:670-74)
Take Home Points
Screening in patients with these disorders (serum IgA and IgA tTG(TG2)) will result in 1-2% positivity (low yield)
But: Patients with a (+) result who are then treated with a Gluten Free Diet will likely likely have response of their skin disorder to dietary restriction of gluten
What about people who are “gluten sensitive?”
There is a group of people who have gone on gluten free diets and say that they feel better. These are people with normal IgA tTG and normal small bowel biopsies. Up to 50 percent of these people do have the high-risk genotype (higher than the 25 percent in normals). A 2012 studied demonstrated that certain symptoms can improve with dietary gluten restriction including GI symptoms, neurological symptoms, skin symptoms and “brain fog” (the most common symptom). These were all patients with a normal intestinal biopsy. (Lundin EA and Alaedini A:Non-gluten sensitivity. Gastrointest Endosopy Clin N Am. 2012. 22: 723-734) A study at the University of Maryland documented that symptoms could be induced by gluten through a blinded challenge that they performed at the university.
In patients with non-celiac gluten sensitivity, adaptive immune response (IgA, tTG, IgE anti wheat and cellular response to gliadin, etc.) cannot be identified. These patients have normal intestinal biopsies and multiple symptoms in response to gluten ingestion that do not occur with placebo. These people may have an innate immune response that can occur in the absence of HLA DQ2. There are also no serologic markers.
Dapsone Treatment
This is the most common question that Dr Zone hears from colleagues. Dapsone is a major oxidant stress to red blood cells. It is important to make patients aware of hemolytic anemia and the blue/gray color associated with methemoglobinemia. Clinical management should stress the maintenance of the smallest dose necessary to control the disease. Occasional new DH lesions (2-3/week) are to be expected, and are not an indication for raising the dose. Before initiating Dapsone treatment, you should perform a baseline CBC and Chem profile; G-6-PD in asians, blacks or those of southern mediteranean descent. You should start your patients at 25 mg. daily and increase 25 mg. weekly until the symptoms are controlled. CBC should be performed weekly for four weeks, then monthly for six months, then semi-annually. Chem profile should be performed at six months and then annually.
https://mauiderm.com/wp-content/uploads/2013/04/MD-WebLogo.jpg00Maui Derm Newshttps://mauiderm.com/wp-content/uploads/2013/04/MD-WebLogo.jpgMaui Derm News2013-12-10 12:07:182014-01-13 08:39:03Gluten: What is all the fuss about? Part 2
Dr Zone has been studying gluten since the 1970s. He comments that recently, all we hear about is gluten sensitivity and gluten free diets. In fact, there are entire sections in the supermarket that are dedicated to gluten sensitivity. This used to be considered rare and now, it appears, that everyone has it. There are now improved methods for diagnosing celiac disease and so the number of people diagnosed has increased. However, there is also a population of people who have self diagnosed gluten sensitivity.
What is gluten?
Gluten is a group of proteins from grains that are insoluble in water. It is made up of prolamins and glutelin. Prolamins are high in proline, alcohol soluble, and monomeric. Glutelin, which we know less about, is soluble in dilute acid or alkali and is comprised of aggregated polymers. Dr Zone mentions that the initial studies feeding people various fractions of gluten were conducted during the 1950s and 1960s, prior to IRBs, “we could feed people a lot of things that we can’t feed people now” and they found that a particular fraction of gluten, the prolamins, were toxic. (The glutelin fraction was never studied) Existing prolamins include gliadin (wheat), hordein (barley), and secalin (rye), all of which may induce celiac disease. Glutenin (wheat), which is a glutelin, may be pathogenic in celiac disease, but this has not yet been confirmed.
Wheat Allergy
In dermatology, we don’t always think about food-induced allergies. Wheat allergy is IgE mediated, i.e., crosslinking of IgE molecules bound to basophils and mast cells. It is repeat sequences in gluten peptides, e.g., serine-glutamine-glutamine-glutamine-glutamine-proline-proline-phenylalanine—not necessarily gliadin. This subsequently releases chemical mediators such as histamine.
The reason why patients with urticaria don’t always respond to anti-histamines is because they are also releasing TNF, proteases, heparin, and IL-5. This is why some people with urticaria will get better with TNF inhibitors.
Wheat Dependent Exercise Induced Anaphylaxis
Dr Zone has seen this on two occasions and it can be quite dramatic. One of his patients had a severe reaction after exercising and they deduced that it occurred because he had eaten gluten; as he didn’t eat gluten before execising, he could continue playing squash. This is caused by omega gliadin and the way to test for this is through a skin test or challenge.
Celiac Disease
Celiac disease is also known as gluten sensitive enteropathy, celiac sprue, and non-tropical sprue. One in 100 Caucasian Americans do have celiac disease. This is an HLA-associated disease. 90 percent of celiac disease and DH patients express HLA DQ2; 9 percent express DQ8. 20-25 percent of Caucasians have DQ2 or DQ8. The receptors coded by the HLA genes are essential for the processing of the gliadin antigen in celiac disease. So if you think about the people out there buying gluten-free foods, 20-25 percent of them have the gene makeup to process the gliadin antigen and develop an immune response. So, essentially, lsss than 5% of the people with the correct HLA genes will develop clinical celiac disease, others may have silent or latent celiac disease and some healthy individuals have all of the genetic makeup to develop celiac disease, yet they will never get it.
It’s important to remember that celiac disease clusters with other autoimmune disorders such as Addison’s disease, autoimmune thyroiditis, atrophic gastritis, SLE, RA, myasthenia gravis, and vitiligo. The interesting thing about this is that we know the antigen that precipitates the autoimmunity. Celiac disease is also common in Down’s syndrome.
Dr Zone comments that it is a “huge mistake” to go on a gluten free diet without first being tested for celiac disease. There is range of pathology in celiac disease that can be seen by proximal small intestinal mucosal immunopathology. Dr Zone also states that he and many of his colleagues were taught that to have celiac disease, you have to have a bloated abdomen, be malnourished and short and skinny…this is how it was described in the past.
What is celiac disease?
Celiac disease is an inflammatory injury of the small intestinal mucosa after ingestion of gluten in wheat, rye, or barley. We can see improvement once gluten is withdrawn from the diet. It is important to remember that many patients with histological inflammation have atypical intestinal symptoms or no symptoms at all. Clinical studies have shown that only 15-20 percent of CD and DH patients identified by serology and confirmed by biopsy have classical symptoms of diarrhea and malabsorption.
So how do you diagnose celiac disease? IgA tissue transglutminase (TG2) is the hallmark of celiac disease and correlates with the severity of intestinal inflammation. A 2003 study looked at the prevalence of CD in the United States based on IgA tTG testing of serum found the following ratios:
1:133 in not at risk individuals
1:56 in symptomatic patients
1:39 in second degree relatives
1:22 in first degree relatives
This demonstrates that CD is common, and not rare. (Fasano et al: Prevalence of Celiac Disease in at Risk and Not at Risk Groups in the United States. Arch Intern Med. 2003; 163: 286 – 292)
Conclusions
Celiac disease is as common as psoriasis and can be found in one to two percent of the Caucasian population. CD profoundly affects the immune system, which is the modulator for inflammatory skin disease.
It is important to remember that most celiac patients have few or no symptoms at all. There is a wide range of intestinal abnormality and the high risk genotype is essential for pathogenesis.
https://mauiderm.com/wp-content/uploads/2013/04/MD-WebLogo.jpg00Maui Derm Newshttps://mauiderm.com/wp-content/uploads/2013/04/MD-WebLogo.jpgMaui Derm News2013-12-10 12:02:382014-01-13 08:40:20Gluten: What is all the fuss about? Part 1
Curtis Cole, PhD, from Johnson & Johnson Consumer Products, is a leading expert on sunscreens and has spent his life’s work on sunscreen technology and formulation. In this presentation, Dr Cole leads a discussion on what every dermatologist needs to know about the current status of sunscreens.
If sunscreens are so good for you, why is there so much noise about it?
Dr Cole mentions the fact that the press and media tend to comment on sunscreen use prior to sunscreen season(s). Many of these comments are read and misinterpreted by consumers and provoke questions around the safety of sunscreens. So what is the truth about sunscreens? Dr Cole states that fundamentally, ultraviolet radiation from sunlight is the major cause of skin cancer. Sunscreens can diminish the amount of ultraviolet radiation entering the skin; therefore, protecting and helping to prevent skin cancer.
Over the last ten years, several papers have been published demonstrating the proof that sunscreen does prevent and reduce skin cancer risk in humans if they are used on a regular basis. (Green A, et al. Lancet. 1999;354:723-729., Heather, L et al. Pigment Cell Melanoma Res. 2010;23:835-837., Adele C, et al. J Clin Oncol. 2011;29:257-263.)
What about estrogenicity and sunscreens?
The SCCNFP is a European “watchdog” group that oversees the safety of UV filters. In a 2001 meeting, the SCCNFP states that “it is of the opinion that the organic UV filters used in cosmetic sunscreen products, allowed in the EU market today, have no estrogenic effects that could potentially affect human health.” There really is no significant estrogenic effect from these UV filters. Studies have shown that estrogenic activity detected in in vitro binding assays did not correlate with in vivo activity. In addition, in vitro binding activity of UV filters are on the order of 1 to 3 million times less potent than estradiol, the standard estrogen compound. Research has also found that UV filters are several hundred times less potent than nutritional sources of estrogen, such as soy or natural supplements.
Does Retinyl Palmitate (RP) in sunscreens increase susceptibility to skin cancer?
The National Toxicology Program (NTP) conducted a nine-year study of RP in albino hairless mouse model. They utilized four concentrations of RP and two of Retinoic Acid and were evaluated against vehicle and untreated controls-solar simulator V source as well as BL and FS lamps. The endpoints were latency period to tumor appearance and tumor yield. Unfortunately this study was flawed; therefore, making the ability to draw a conclusion difficult if not impossible. The study was flawed for several reasons including:
Vehicle utilized 15% isopropyl adipate, a potent penetration enhancer
The top two concentrations of RP were toxic and had to be eliminated from the study
The “enhancing effect” of the vehicle over the untreated but irradiated mice was equivalent to 200% increase in the UV dose
The effect of RP was only evident in one gender of the mouse model and not the other
The results are contrary to human evidence that retinoids are chemoprotective to skin cancers. The NTP is considering redoing this study in order to achieve results that are more accurate.
Nano Materials in Cosmetic Materials
Nano materials are much more efficient in blocking UV and they are much more cosmetically acceptable. There are hundreds of papers that are published looking at the “nano sizes” questioning the penetration of TiO2 and ZnO particles. A recent paper by the FDA demonstrated that they could not find penetration from these nano-sized particles. A paper from Sayre R, et al. looked at whether “physical blockers” really act differently than “chemical” UV filters. They found that ZnO and TiO2 actually have a semiconductor energy band gap and absorb UV with the same mechanism as “chemical” UV filters. The “transparent” micronized inorganic filters have little scattering effect, if they did, they would be very visible on the skin. (Sayre R, Kollias N, Roberts R. Physical sunscreens. J. Soc. Cosmet Chem; 41:103-109)
What about inorganic (mineral filters)?
Are they better than organic (chemical) filter-based sunscreen? Dr Cole states that there is a much higher level of absorbance among the organic filters because the chemical filters are much more potent. Dr Cole is not saying that the physical filters are not useful, they do; however, have a place for patients who cannot tolerate the organic filters. Also of note, the organic filters are much more aesthetically pleasing.
Do you really have to wait 15-20 minutes for sunscreen protection?
Sunscreen testing protocols mandate drying times of 15-20 minutes before SPF testing can begin; the mandatory labeling reflects this instruction. Actually, UV protection is instantaneous. However, it is important to remember that water resistance may require more drying time. All of the sunscreens that claim water resistance have a type of polymer that is set up to be a barrier against the water. Reapplication (every two hours) of sunscreen is another key component of preventing/reducing sunburns, in fact this is mandatory labeling by the FDA. A paper in 2001 surveyed 57 people on a beach in Texas. Out of these subjects, there were at least 50 people who got sunburned on the beach; those who do not get sunburned re-applied their sunscreen every two hours. (1Wright M, Wright S, Wagner F. Mechanisms of sunscreen failure. J Amer Acad Dermatol. 2001;44:781-784)
Current Misconceptions on High SPF
Dr Cole asks the question of whether SPF 100 is really better than SPF 50. Here are the facts: SPF 100 blocks 99% of damaging UVR and SPF 50 blocks 98% of damaging UVR. Therefore, 1% of SPF 100 is getting through the filter and 2% of SPF 50 is getting through the filter. This means that it is the amount getting through the filter that matters. It’s not so much what you block, it is how much gets through. It would take twice as long to get the damage with SPF 100 than what you get with SPF 50.
Numerous studies have demonstrated that consumers typically under apply sunscreens. Higher SPFs can help compensate for under-application as SPF protection is directly proportional to the amount applied.
How does all of this information affect the products and labeling?
Most sunscreen products were unchanged
High SPF products (>SPF 50) still allowed
What did change?
All products now labeled with drug facts box
Test method for broad spectrum claims final – CW
Broad spectrum claims not allowed for products with SPF<15
Statement recognizing use of sunscreens for skin cancer prevention and skin aging is permitted (with an SPF of at least 15 and/or Broad Spectrum)
Broad Spectrum
Broad Spectrum is determined based on “critical wavelength” in vitro absorbance calculation, i.e., wavelength below which 90% of the absorbance is present. 370nm is the “pass/fail” critical wavelength for “Broad Spectrum Protection.” It is important to remember that critical wavelength measures the breadth of protection, yet it does not measure the magnitude; therefore, critical wavelength does not always correlate with UVA protection. The ability to achieve a critical wavelength of 370 becomes more and more difficult as SPFs increase above 30. Dr Cole recommends looking for products with an SPF:UVA-PF ratio of less than 3:1 (which is a requirement for European sunscreen products).
Individuals Particularly Sensitive
Patients/Consumers who are need of the best available protection are those who are highly sensitive (Phototypes I and II, photosensitive conditions and patients on immune suppressive drugs and those who have skin cancers. Others who are also in need of good protection are those who want to limit further photodamge, fine lines, wrinkling and pigmentation.
Why use a high SPF?
Extreme conditions of exposure warrant a higher SPF. These are conditions such as high altitude and those of high reflectivity such as ocean surface, sand and snow. In a controlled consumer trial (split-face, double-blind design) of 56 people at 8500 feet with all day sun exposure demonstrated that more individuals had sunburn using an SPF 50 versus an SPF 85 product. (Rigel et al. 2009. J Am Acad Dermatol;62, I:2:348-349)
Testing of high SPF products has been validated up to SPF 90. A controlled, randomized, multi-center trial was conducted using SPFs 16, 70 and 90 and four test laboratories using multiport and singleport solar stimulators. The results showed that all of the SPF levels could be distinguished from each other in the four labs; yet, no significant differences in SPF values of each product between laboratories. The testing demonstrated the ability of the laboratories to determine high SPF values with accuracy and reproducibility. (Stanfield, Ou-Yang, Chen, Cole, & Appa. 2011. Photodermatology, Photoimmunology & Photomedicine ;27:1,30-35)
Sunscreens and Squamous Cell Carcinoma and Malignant Melanoma
A randomized controlled study in Australia looked at sunscreen use (daily versus discretionary), risk of BCC and SCC (and melanoma). Use of an SPF 16 product and weight of the product brought in was measured every three months. The researchers found a significant reduction in the risk of SCC (RR 0.61; 95% CI 0.46 to 0.81). This suggests that melanoma may be preventable in adults with the regular use of sunscreen. (Green AC, et al. J Clin Oncol. 2011;29(3):257-263.)
Conclusions
Skin protection from damaging sunlight requires a multi-layer defense. Sunscreen should be part of the overall plan for protecting from sun damage. It is important to avoid unnecessary sunlight and you should avoid highest UVB intensities of sunlight (10am-4pm). Skin should be covered with clothing and a hat and high SPF should be used for skin that remains exposed.
https://mauiderm.com/wp-content/uploads/2013/04/MD-WebLogo.jpg00Maui Derm Newshttps://mauiderm.com/wp-content/uploads/2013/04/MD-WebLogo.jpgMaui Derm News2013-12-10 11:57:262014-01-13 08:42:26Debunking the Myths of Sunscreen
In the world of dermatology, we are filled with hamartomatous “overgrowth” syndromes. Many, however, are de novo so the genetic mechanism is unclear. Often times, segments or large quadrants of the body are affected clinically suggesting somatic mosaicism.
Two studies in 2012, that complimented some earlier studies, looked at somatic mosaic mutations of these various overgrowth syndromes. In the first study, megacephaly was a feature in all three cases. Patients may have nevus flammeus. The blood/saliva from all patients was subjected to total exome resequencing, which is a technology that is really hitting medicine right now. In effect, total exome resequencing is looking at all of the coding sequence of one’s genome (exome) and in doing so, trying to find the mutation that may be responsible for the phenotype that you see. In the first study, megacephaly was a feature in all three cases. Patients may have nevus flammeus.
The three genes that were found were the AKT3, PIK3R2, and PIK3CA.
Clinical Pearls
Germline and mosaic versions of cancer mutations lead to developmental and hamartomatous conditions
As sequencing technologies improve, the mechanism of new syndromes will emerge
Interesting that these patients may not be more susceptible to cancer overall
Looking Ahead
Between biologics and small molecule inhibitors, we are in a new therapeutic renaissance
The mechanism-to-medicine bridge is finally open
NextGen sequencing will help define rare hereditary and mosaic genodermatoses
Health care economics, not science, is the wild card
https://mauiderm.com/wp-content/uploads/2013/04/MD-WebLogo.jpg00Maui Derm Newshttps://mauiderm.com/wp-content/uploads/2013/04/MD-WebLogo.jpgMaui Derm News2013-03-15 19:31:512014-01-13 10:38:04Dermatology Year in Review Part 3: New Insights
Dermatologists should remember that most basal cell carcinomas (BCCs) are removed by surgery or with radiation or topical therapies. This past year there has been much more data on hedgehog signaling, which is involved in most BCCs.
Hedgehog Pathway
Vismodegib, which targets the hedgehog pathway, has been studied in BCCs. Of note, the hedgehog pathway is also being studied in other cancers, including pancreatic and brain cancer.
Sekulic, et al. published a study in the New England Journal of Medicine looking at the efficacy and safety of Vismodegib in advanced basal-cell carcinoma looking at 33 patients with metastatic basal-cell carcinoma and 63 patients with locally advanced basal-cell carcinoma, the latter of which is more prevalent in the dermatology setting. The primary endpoint of the study was independent review by an outside dermatologist. The study concluded that Vismodegib is associated with tumor responses in patients with locally advanced or metastatic basal-cell carcinoma.
The most commonly reported adverse events (AEs) were muscle spasms, alopecia, and dysgeusia. Other AEs included decrease in weight, fatigue, nausea, decrease in appetite, and diarrhea.
Tang, et al. studied the results of inhibiting the hedgehog pathway in patients with basal-cell nevus syndrome. (New England Journal of Medicine) There were 41 patients in the study; 26 on Vismodegib vs 15 on placebo. The study looked at cessation of new BCC development while on Vismodegib and the decrease in the diameter of existing lesions while on Vismodegib.
The data from this study demonstrate that one can see no new BCCs form while on Vismodegib and a significant decrease in the diameter of existing lesions while on drug. (Of note, there was a significant attrition of use because of the side effects.) Also of importance is the fact that GLI1 levels diminished on patients taking Vismodegib; therefore, indicating that the drug is hitting its target.
Clinical Pearls
This small-molecule hedgehog pathway inhibitor is effective for metastatic, advanced and generalized BCCs
Represents nice bench-bedside development of a new cancer agent
Side effects, recurrences after drug discontinuation, and cost are limiting factors
Although FDA-approved, the role of Vismodegib for common BCC settings is unclear given limitations
Head Lice
The emergence of resistance to first line antipediculicides complicates the public health problem of head lice. Dermatologists should remember that second-line treatments, such as lindane and malathion, have limitations related to safety; therefore, newer approaches for the treatment of head lice are needed.
David Pariser and colleagues published a large prospective trial in 2012 in the New England Journal of Medicine looking at topical Ivermectin 0.5% for the treatment of head lice. The study found that Ivermectin has a higher success rate versus the control vehicle.
The side effects for Ivermectin were rather tolerable. AEs included pruritus, excoriation, and erythema.
Topical ivermectin achieved a success rate of >90% with single application
Similar to oral ivermectin
Nit combing not necessary with ivermectin as opposed to permethrin
Nice option for permethrin-resistant louse or even as first line
Targeted Therapy for Melanoma
Although molecular control of melanoma through targeted therapies has shown tremendous success, relapse is still the general rule; therefore, long-term remission will require immune participation in order to have recognition at the immune surveillance level. Often times, the tumor evades the immune system by circumventing immune checkpoints; yet, recent advances in the studies of targeted therapy for melanoma (Anti-PD-1 and Anti-PD-L1 antibodies) have demonstrated positive efficacy in tumor reduction.This new area of research is at the level of the tumor itself. These therapies, currently under trial, both have major potential in clinical practice and patient outcomes.
Data from Topalian et al, published in the New England Journal of Medicine show that the objective response rates are less than 30 percent as defined by the RESIST criteria. Many patients experienced a drop-off of greater than 30 percent tumor reduction using anti-PD-1. The anti-PD-L1 shows similar results, but not to as great as an extent as that of anti-PD-1.
Clinical Pearls
Anti-CTLA4, anti-PD-1 and anti-PD-L1 represents the triumvirate of immune checkpoint therapies
Precise molecule and formulation may be important
Tremelimumab (another anti-CTLA4 antibody) did not show any significant survival benefit
Anti-PD-1 and anti-PD-L1 treatments appear to be less toxic than ipilimumab
Combination molecular therapies for acute control and checkpoint therapies for long-term control may be the wave of the future
Overcoming Rejection and Cancer
A small study in the New England Journal of Medicine looked at the role Sirolimus (rapamycin) in secondary skin cancer prevention in the transplant population. Rapamycin, which targets the mTOR pathway, blocks the transduction pathway. This action not only prevents the rejection, but can also prevent SCC from developing.
Patients in the study were randomized to either Sirolimus or cyclosporine, tacrolimus. All patients had at least one prior SCC and were stratified by the number of prior SCCs. Overall there was a significant improvement in the probability of survival-free with Sirolimus compared to the calcineurin inhibitor controls. However, when the data is broken down, one can see that the majority of this effect occurred in the sub-population, i.e., patients with only one prior SCC.
Clinical Pearls
Sirolimus is an effective suppressor of transplant rejection and has the added benefit of suppressing development of SCCs
The medicine’s positive effects must be balanced against a large number of adverse effects
It is less effective in patients who have already had more than one SCC
This is not the final word in prevention of skin cancer in transplant recipients
https://mauiderm.com/wp-content/uploads/2013/04/MD-WebLogo.jpg00Maui Derm Newshttps://mauiderm.com/wp-content/uploads/2013/04/MD-WebLogo.jpgMaui Derm News2013-03-15 19:29:432014-01-13 10:40:20Dermatology Year in Review Part 2: New Treatments