Social Media
Jeff Benabio, MD
At MauiDerm 2014, Dr Benabio provided an overview and update on Social Media and its potential use in clinical practice…
Did you know that Yelp is a social media website? It is and for doctors, this is something that you should know. Why does the New York Times pose questions at the bottom of their posts? They do this in order to engage their customers and it turns out then when people participate in your brand, the lifetime value of that customer goes up. This is very much what is happening with social media.
The What, Why and How of Social Media
Remember that social media is a lot more than just Facebook! Social media is digital technologies that allow us to connect and share things/ideas with each other. This is a core human capability, i.e., connecting with people. The internet, in its entirety, is essentially a social media site. This is important because it changes the way we interact as a society. Dr Clay Shirky, a Professor of Communications at NYU, suggests that there were four innovations that fundamentally changed society. These are 1. The printing press; 2. The telephone and the telegraph; 3. Radio and television; and 4. Social media.
114,700,000 people watched the SuperBowl in 2013, it’s the largest television event of the year. On Superbowl Sunday, 650 million people will be on Facebook and on Monday, and Tuesday, etc.. That is to say, 650 million people are on Facebook every single day. That’s six times the Superbowl viewers. Four billion YouTube videos are watched every single day. This is the power of social media. This is very important for us, as healthcare providers, because not only are we in medicine, we are a small business.
This is all part of marketing. When we talk about marketing we think about advertising, the vision and culture of our practice, i.e., the needs of the patients, sales, and online/mobile presence. Whether you want to or not, you have an online presence. You have to build brand awareness. Marketing today is no longer one-directional it is bi-directional. In marketing terms, “bi-directional” means the consumer can communicate with the business. Newspaper ads are unidirectional, that is, the patient reads it and cannot respond. A YouTube video is bi-directional because it allows the user to communicate with you.
There are four stages to marketing communications:
- Awareness: To capture their attention about a specific product or service.
- Information: To convey factual information about a product or service.
- Attitude: To persuade them to change their attitude regarding a brand.
- Call-to-Action: To persuade them to act through specific behavior (purchase your products, make an appointment, subscribe to our blog or newsletter)
How do we get most of our patients? Word of mouth is the number one way. How are patients getting word of mouth now? They find this information on the internet. In 2012, Deloitte found that 52 percent of patients used the internet to learn about doctors. Of those who use the internet, they spend, on average, two days researching before they make the decision to come and see that doctor. This is the good for us. We want patients to trust us. 2012 Neilsen Global Trust in Advertising found that 92 percent of consumers say they trust “earned media” including recommendations from family and friends above all other forms of advertising.
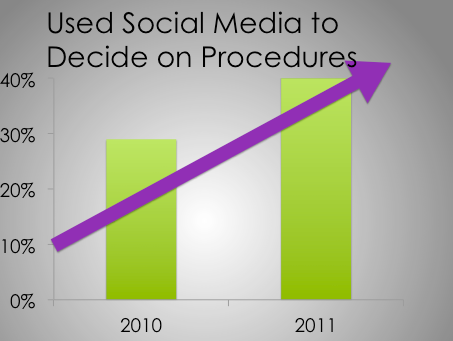
The American Society of Plastic Surgeons conducted a study looking at patients and the influence of social media regarding decisions on surgical procedures. In 2010, 29 percent of patients utilized social media that figure rose to 42 percent in 2011 and the numbers continue to increase.
We are beginning to see websites like Vitals where patients can find doctors or facilities and write reviews. Vitals is a doctor rating site. They are trying to communicate that they are a trusted source. This is a great opportunity for us as physicians. We can’t necessarily operate on a site like Vitals, but we can on a website such as Health Tap. Health Tap is a question and answer site, i.e., people ask questions and experts answer them. When you answer the question, you get stars next to your name. 50,000 doctors went online to answer over a billion questions. This is an opportunity to demonstrate to patients that we are a trusted source. We are able to not only market to patients, but we can deliver something of value to them. These sites are very fast growing, particularly among providers.
RealSelf is another website similar to Health Tap; however, it is specifically for cosmetic surgery. RealSelf has 36 million unique visitors and there are 500,000 answers from board-certified physicians and healthcare professionals. Two hundred and thirty nine million dollars were spent by Real Self users on cosmetic surgery. This is a community that connects eager patients with trusted, vetted physicians. Their goal is to educate patients so that they can make informed decisions about cosmetic procedures. They post pricing on the website as well. This is an important trend that patients want to know about it as patients want transparency.
Eighty percent of people go online to search for health information. What do they see? If you Google yourself, you may find that you’re competing with restaurants and other reviews. “Is she or he a good doctor?” is a difficult question to answer. This is often substituted with “do I like him/her?” If you think that review sites are going away, that’s not true. This is a good thing. If you’re doing the best thing(s) for your patients, these websites are going to help you. These websites work and patients get something out of them. You need to demonstrate this to your patients.
What can I do on my review site(s)?
Post a picture of yourself so that your patients can see you. Make sure that the information about your office/practice is accurate and say something personal about yourself. Patients are looking for personal information that connects you with them. This is free points for you and patients really care about it. You want to convey that you and your practice care about your patients. People want the “Apple” store experience when they come to see you.
What about Pinterest? Pinterest, if you didn’t know, is a tool that consumers use in order to find information on ideas and projects. There are 70 million users and 80 percent are females. This is important for us because 80 percent of women are the primary healthcare decision-makers among families. This is a great place to interact with women who are shopping. This is what women are interested in and it is an ideal place to showcase services. Harvard Business School refers to this as “reverse showrooming.” Reverse showrooming refers to when people browse online then purchase in a store. Pinterest is a big driver on in-store sales. 21 percent of users said they bought an item in-store after pinning, repinning, or liking it, and 36 percent of users under 35 said they had done so.
What about Facebook? What do people do on Facebook? Facebook is about feeling something. People go online to share pictures and talk about their families. If you go on Facebook, you have to be very careful about advertising. What about Twitter? Twitter is about now and relevance. What about YouTube? YouTube is a great place to convey information in an efficient manner. You can deliver value about a service. “If there’s anything more annoying than people talking about you, it is to have no one talk about you.” Oscar Wilde
Remember that social media is just one type of marketing. You should be using it along with traditional media and marketing tools. If you think social media is important now, wait until the next generation.