Melanoma Clinic: Lunch, Lesions, and Lessions
Part 1
Hensin Tsao, MD, PhD
Keith Flaherty, MD
Ilona Frieden
Philip LeBoit, MD
Dr Hensin Tsao, of Harvard Medical School, discusses several challenging cases with regards to the management of melanoma and pigmented lesions…Remember that melanoma, as an area, is not always easy.
Case 1
A ten year-old girl presents with a pink plaque on the left shoulder. The lesion has been present for four months and she has no other medical problems.

As a clinician, what would you do next?
- Photo and follow up in 6 months
- Reassure and continue careful surveillance at home
- Perform an excisional biopsy with local anesthesia
- Biopsy under general anesthesia
Why not photograph and follow or reassure and continue surveillance. Because of the shape of this lesion, it’s a little bit bigger than normal spitz nevus. Because of her age, she can probably tolerate anesthesia so it would be worth obtaining a good specimen. The biopsy showed 1.5mm thick, Clark level IV, it was non-ulcerated and 2 mits/mm2.
Managing Pediatric Melanoma
A study by Cordoro and colleagues demonstrated that pediatric melanoma does not follow the ABCDs. What do we look for? Most teenagers who get melanomas get adult-type melanoma. Up until age 13, melanoma is diagnosed at a relatively low level. Amelanotic or bleeding is also more frequent presentations of melanoma in younger kids.
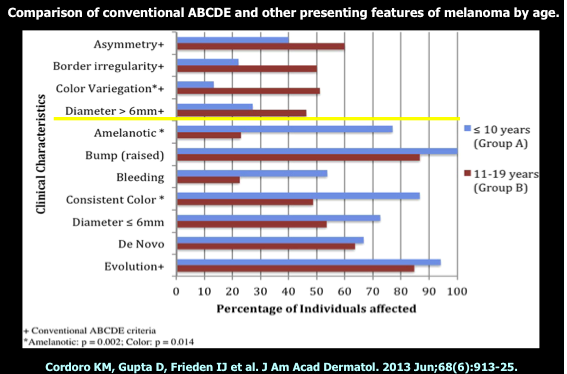
ABCDE Modified for Children
- Amelanotic
- Bleeding; bumps
- Color uniformity
- De Novo; Diameter; any
- Evolution
Make sure that you have a dermatopathologist with whom you are very confident!
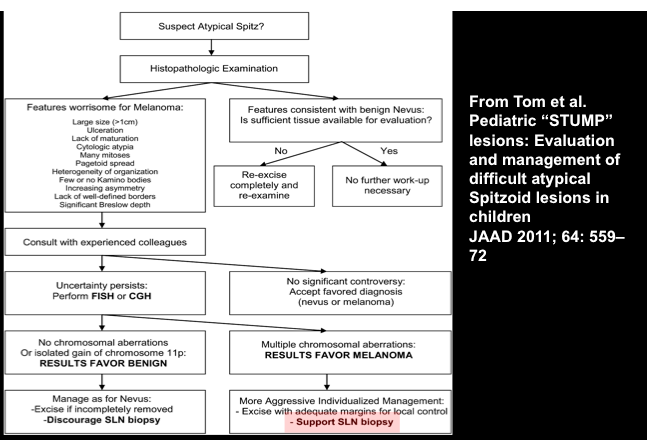
Risk stratification, rather than black and white diagnosis, is the way things are going now with regards to tumors and general pathology. There are lesions where we cannot always make a precise diagnosis, even after molecular testing. In many of these cases, all we can say is that it is a Spitzoid neoplasm with very low or high malignant potential. Spitzoid neoplasms can be stratified into four categories. These are Spitz nevus, Spitz nevus with atypical features, atypical Spitz tumor and Spitzoid melanoma. Bastian and his colleagues have developed Spitzoid taxons:
- H-ras mutated
- Bap-1 mutated
- Braf fusion
- Alk fusion
- Ntrak1 and ntrak3 fusion
- Ros-1 fusion
One very interesting concept is that many of these genes, if you take them and translocate them in cells other than melanocytes, they are extremely potent in terms of oncogenic effect. ROS-1 and Alk, for example, are important players in lung cancer. Mutations or fusion partners do not define benign versus malignant, but only lineage. So, doing a test for Alk will not tell us if the lesion is benign or malignant; however, if the lesion does metastasize these are very important venues for therapy. For instance, BRAF, even though there’s no Braf mutation in these lesions, it is over-expressed and anti-BRAF therapies may be effective in Spitzoid melanomas that have a BRAF fusion. You don’t have to have the mutation for BRAF inhibition to work, if it’s a tumor where other things are turning it on.