
10 Pearls About Pigmented Lesions
Whitney A. High, MD, JD, MEng
Dr Whitney High provides us with ten clinical pearls about pigmented lesions from the dermatopathologist’s point of view…
- There are distinct histologic differences between wholly bland nevi, and what has come to be known as an “atypical nevus,” a “dysplastic nevus,” or a“Clark’s nevus.”
- There is no single criterion (not even mitoses or pagetoid spread) that is diagnostic of only melanoma. There is not a “melanoma stain” that wholly discriminates between atypical nevi and melanoma. “Borderline” lesions represent subjective assessments that are impacted by the viewpoint and skill of the examiner.
- Biopsy use is increasing. In nine geographic areas of the USA, over 1986-2001, the biopsy rate among those persons >65 years of age rose 5-fold, while the melanoma rate rose 2.4-fold.
- In many areas of the country, atypical nevi are graded “mild,” “moderate,” or “severe,” but this is not universally employed. Some dermatopathologists “lump” mild and moderate together, and have just two categories. In other areas of the county nevi are not formally graded, or are graded in a less straight-forward way (i.e. “nevus,” “Clark’s nevus,” and “Clark’s nevus, re-excise”).
- The dermatopathologist is examining only a small portion of your biopsy, and this must be considered with regard to the “representative” nature of the results. A 2010 study showed the odds of misdiagnosis for pigmented lesions were considerably higher when a punch biopsy technique was employed in comparison to an excisional biopsy (see: Ng et al. 2010).
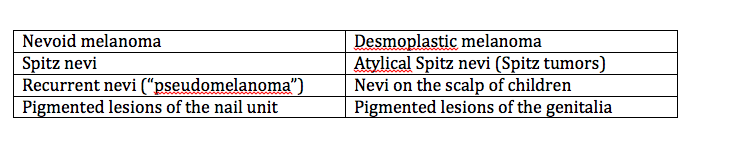
- There are special situations where the diagnosis of melanoma is challenging, such as:
- There are some immunostains that can “assist” in the assessment of melanoma, or “bolster” the one’s confidence in a diagnosis, and these include: Mart1/Ki67 (a combination stain), P16, and HMB45, but again, there is, however, no singular “melanoma” stain.
- Spitz nevi, in particular, may be confused with melanoma, and vice versa. Generally, if the patient is older than 20 years of age, it is wise to ensure that the dermatopathologist examining a case of a Spitz nevus or spitzoid melanoma has experience with difficult pigmented lesions.
- Desmplastic nevi may be difficult to distinguish from other malignant processes (such as an atypical fibroxanthoma or spindle cell squamous cell carcinoma), and desmoplastic melanoma may also be confused with simple scarring, particularly in a shallow specimen. Stains and careful examination may often be employed in such a case.
- Synoptic reporting (a “grid-like” summary) of characteristics that allow for the pathologic staging of melanoma is an emerging standard in dermatopathology, and probably more rapidly and more accurately transmits key therapeutic and prognostic information to the clinician.